Most healthcare organizations budget the same way they did ten years ago: last year’s numbers plus a percentage adjustment, built in Excel, distributed to department heads who accidentally break it, then stitched back together over a stressful weekend before the board meeting.
It works. Until patient volumes shift 12% in a quarter and your static budget has nothing useful to say about what that means for staffing or supplies. Then an auditor asks you to trace a six-figure variance across three facilities and your answer involves opening nine spreadsheets and hoping the links still work. The consolidation that was supposed to take an afternoon takes a week because someone inserted a column in the wrong workbook. And at some point you realize you have not reforecasted since January because the process is so painful that everyone quietly agreed to skip it.
Healthcare budgeting is genuinely harder than budgeting in most other industries. But a lot of the pain finance teams experience is not actually caused by the complexity of healthcare. It is caused by tools that were never built for this job.
Patient volume. That is the answer to most healthcare budgeting questions and the source of most healthcare budgeting headaches. A manufacturing company can forecast demand from contracts. A SaaS business can model growth from pipeline data. But a hospital budgets around a variable it cannot predict or control, and that variable drives everything: revenue, staffing ratios, supply consumption, overtime costs, capacity utilization. Get the volume assumptions wrong and every downstream number inherits the error.
Flu season creates predictable spikes. Elective procedures dip around holidays. But a new urgent care clinic opens two miles away and your outpatient volumes drop 8% overnight. A payer renegotiates reimbursement rates mid-year. A global health event reshapes demand patterns for months. None of that shows up in a budget built from last year’s actuals plus 3%.
The departmental complexity compounds this. Pediatrics, radiology, surgery, pharmacy, lab, nursing, admin, each with its own cost drivers and budget owners, all needing to roll up into a consolidated view that leadership can trust. Shared services like IT and HR need to be allocated across all of them using methods that hold up under audit. Managing that many interdependent budgets in interconnected spreadsheets turns your consolidation into a source of risk rather than clarity.
And regulators are watching all of it. Every allocation needs documentation. Every variance needs an explanation. Medicare cost reports, state mandates, and grant compliance all demand financial data sliced in specific ways. If your budgeting process cannot produce those views without hours of manual reformatting, that is an operational risk you are carrying every day. The audit trail requirement alone disqualifies most spreadsheet-based processes.
Most healthcare organizations default to incremental budgeting because it is fast. Adjust last year’s numbers, distribute for input, consolidate, present. The problem is that it bakes in whatever inefficiencies existed last year and never asks whether the spending pattern still makes sense. If a department was overspending, that overspend becomes next year’s baseline.
Zero-based budgeting fixes that by requiring every dollar to be justified from scratch, but it takes far longer. Doing it across a multi-facility system every year is not realistic for most teams. Activity-based and driver-based approaches tie costs to operational metrics like patient days and procedure counts, which makes reforecasting much easier. Change the volume assumption and costs adjust automatically instead of requiring a manual rebuild. The right answer for most organizations is a blend: incremental for stable areas, driver-based for anything sensitive to volume. But here is the thing most budgeting approach discussions skip: the approach matters less than whether your tools can actually support it. A brilliant driver-based model is worthless if one misplaced formula corrupts the output.
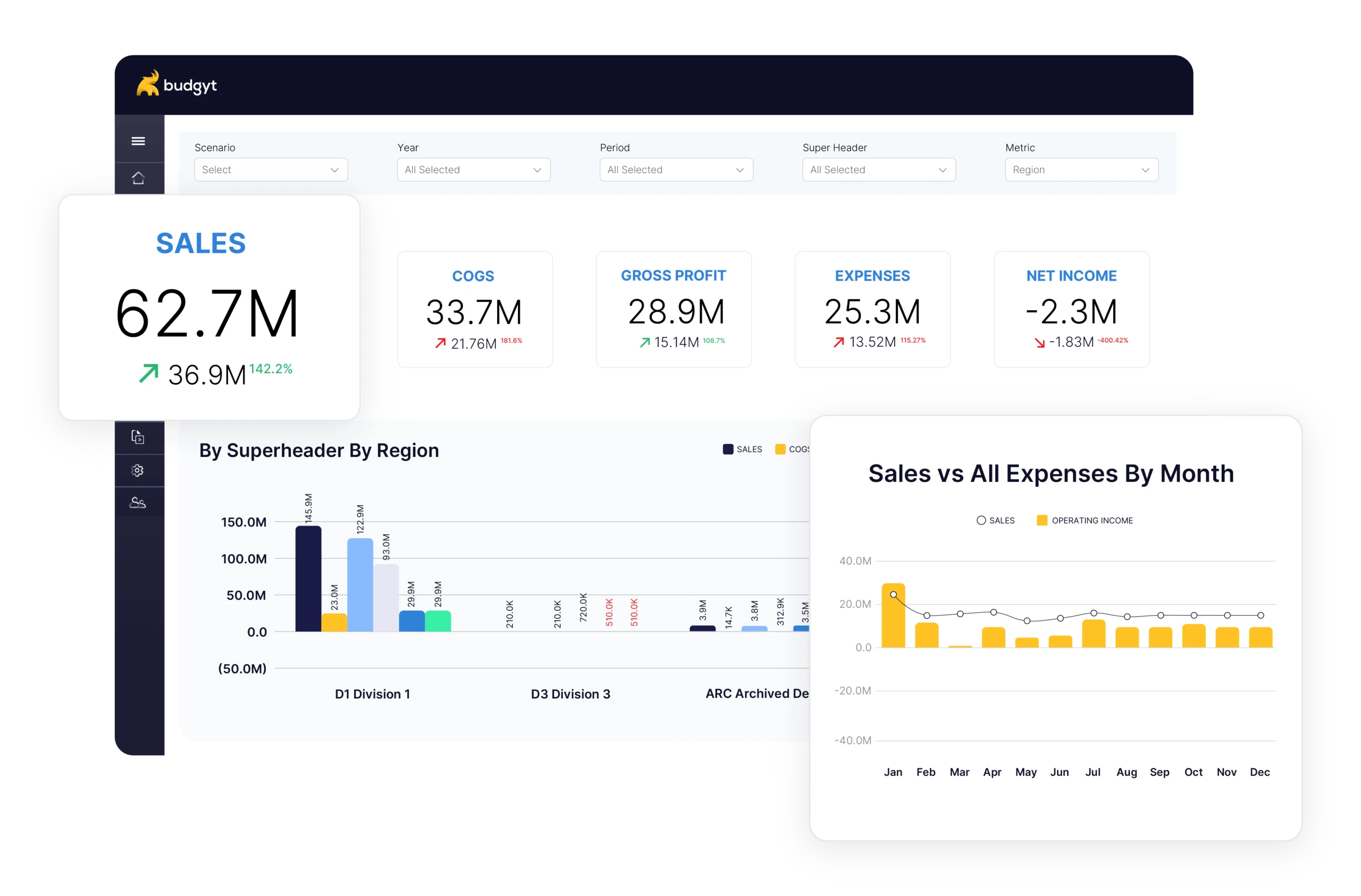
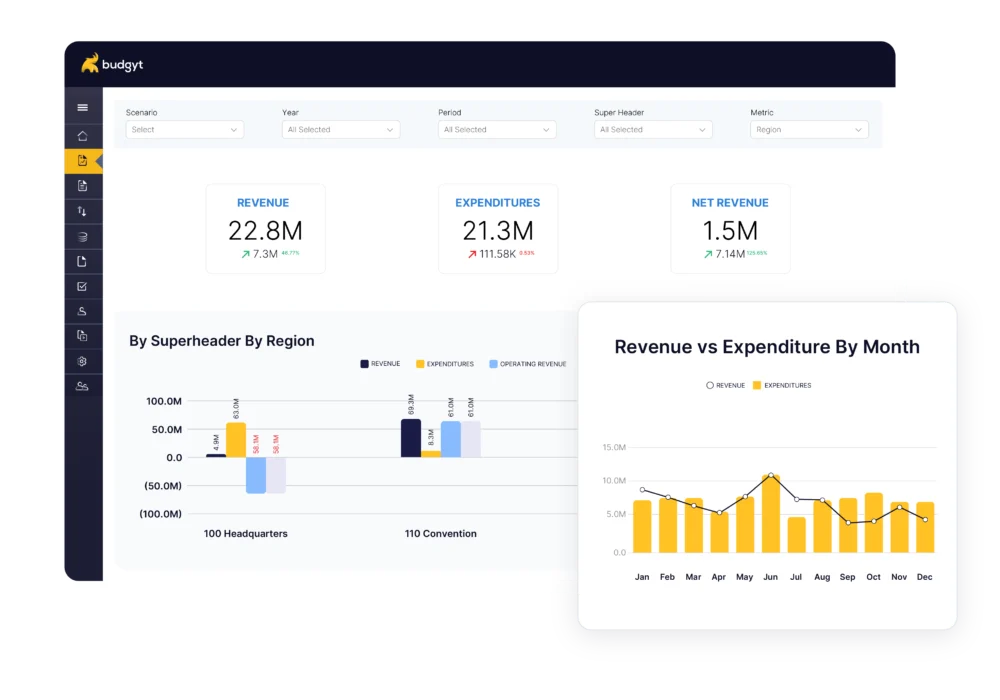
Remember the consolidation problem from earlier? Budgyt was built to make it disappear. The platform runs on a database, not spreadsheet formulas, so your calculations hold up no matter how many people are contributing data or how often assumptions change. Contributors work in their own sections without any ability to alter the underlying model. You get real collaboration without the version control anxiety.
For healthcare organizations, that means site-level and system-level reporting that consolidates automatically, cost allocation across clinical and administrative departments, volume variance analysis, census-driven reforecasting, and a complete change log that satisfies audit requirements. Select any number and see what is behind it: which site, which department, which line items. No more reconstructing the logic after the fact. Budgyt connects to QuickBooks, Sage Intacct, NetSuite, Dynamics 365 Business Central, and Xero for ongoing actuals import, so your variance analysis runs on real data rather than manual re-entry.
A mid-sized healthcare organization brought eight departments into one collaborative process after switching. “We’ve been using Budgyt for the past two years, and it has completely transformed the way we manage our budgeting process… Budgyt has streamlined everything, making it efficient and straightforward.” They scored Budgyt 10/10 on TrustRadius.
If your current process involves separate files for every facility, a consolidation phase that takes days instead of minutes, or a reforecasting cadence of “we should do that more often but don’t.” Those are the signals. Book a demo to see how Budgyt works with healthcare data, or start a free trial and connect your accounting platform to explore with your own numbers.
Do not try to migrate everything at once. Pick one facility and rebuild its budget. See how it feels when the formulas cannot break and the audit trail builds itself. Get your department heads in the system and let them experience the difference between contributing to a protected model and being handed a spreadsheet they can accidentally destroy. That is usually enough to settle the question of whether the switch is worth it.
You manage millions of dollars. You make decisions affecting dozens of employees. You report to boards with fiduciary responsibility.